|
Here we are at 5 Weeks + since my surgery! All indications are that recovery is going very well. And, I think it’s time to celebrate some victories in this process.
First, a win for something that didn’t happen: There have been no issues of VPI or hypernasality in my speech since the surgery. As you may recall from my pre-surgery posts, there was a concern that the advancement would stretch the pharyngeal flap and create conditions for VPI. My voice sounded pretty good even right after the surgery, but my surgeon cautioned us that congestion due to post-surgical swelling could obscure VPI. The swelling is now almost entirely gone, and still no VPI. I think we can call this a wonderful success. I have occasionally shuddered to imagine an alternate reality I could have experienced: struggling through that recovery while dealing with the trauma of realizing that my voice had reverted back to the nasality I began with as a small child, the self-consciousness of sounding like – as they labeled me then – a “crippled” person once again, and the knowledge I would have to go through therapy and possibly more surgery to correct it. Thankfully, this did NOT happen. And I must hand a great deal of the credit for that to my surgeon’s skill and care. Thank you, Doctor. Another victory is the fact that I’ve been able to re-assimilate into my musical work. I’ve had several rehearsals with Choral Arts Northwest, and will be singing the Duruflé Requiem this Sunday in concert. My singing voice is not 100%, but I can sing with decent tone and moderate power in the mid-range especially. In another victory, I’ve led three rehearsals with one of my choirs, the Skagit Valley Chorale. This group has well over one hundred singers this semester, and we have made an accommodation to help make sure I will be heard by everyone without straining: I am using a lavaliere microphone through a p.a. system. It is working very well. I think people can hear better than in rehearsals in the past – and I have been relieved at not having to worry about being heard. There is another victory whose possibility I have sensed, but not confirmed. With the advancement of my mandible and maxilla, it seems logical that both my pharynx and my mouth have greater volume. I have had the impression a few times when I have sung that I now have a larger resonating space for my voice – but I haven’t been able to really test this yet, for several reasons. My face is still numb and I don’t feel that I have good control over various muscles involved in singing, especially regarding changing vowels and changing formants. My hard palate area is still somewhat numb and doesn’t report reliable information about the sensations of resonation that I am used to. Also, I am not supposed to do vigorous activity, and full-power singing is a vigorous activity. I’ve found that the more power I put into my singing, the more it irritates the paresthesia in my face. I believe that the vigorous activity of singing can put pressure – similar to sneezing, straining, bearing down, and other activities I’m not supposed to do – on my healing facial bones that is not good for bone recovery, including the “bony union” at the advancement sites. As my surgeon releases me from limits on activity, and as my paresthesia begins to ebb, I’ll be able to explore this some more. I’m interested to see what my upcoming tests at the UW Speech and Hearing Clinic will show compared to the “before” tests we did in July. Anyway, I have a quiet and perhaps not-unfounded hope that I’ll find I have a richer tone than I did before the surgery. That would be exciting! The final victory that I’ll mention right now is just the recognition that my recovery continues to go well. One part of that victory is that I’m living with paresthesia day to day without freaking out about it. :) I trust it’s going to heal in time. Another is that I’m doing well at feeding myself, and not wasting much time being self-conscious or annoyed about realities like having to take lots of time preparing food, eating with a mirror and catching the dribbly bits that run down my chin, and drooling at any moment without knowing it (oh, joy). Friends, family, fellow musicians have been tremendously supportive, my spirits are good, and I seem to be handling the things I need to be doing, personally and professionally. May it continue so! Looking to the future… As you will have noticed, it’s been a while since I made a post. My music career – relatively quiet (hah!) during the summer – has picked up again with rehearsals and project management and study. One result of that is that I don’t have the same amount of time to write blog posts. Lorraine reminds me that if a blog is not updated on a regular basis, people stop checking it and readership goes way down. Yes, I know this to be true, and I accept it; I just don’t have the time to post regularly. The main impetus for this current spate of posts – my surgery and recovery – is winding down as my work winds up for the year. I’m certainly planning to make more posts – more about paresthesia, more about eating, and I’m sure other things like my upcoming work with speech therapy. But they will be fewer and farther in-between. So I’ll thank my readers who have gone on this journey with me, and say I’ll be back from time to time. Also, it has always been my intention that this blog will develop into many more areas of interest than my surgery and recovery. I look forward to finding out what’s going to inspire or prompt me to post!
3 Comments
Yes, Mark Watney, the fictional hero of the book The Martian by Andy Weir, is a man who inspires me to be a better person. I wrote most of this post in my head two weeks ago, much earlier in my recovery, and just hadn’t gotten around to writing it out and posting it. But, tonight I finished listening to the audiobook and am inspired to give credit where credit is due: to author Andy Weir, to R.C. Bray, who read the audiobook, and to their creation, Mark Watney.
I’ve been listening to the book since my first day in the ICU after my surgery. In the first two weeks of my recovery, Mark Watney was my regular companion and helped me keep perspective. Thinking I had it bad? Mark had it much worse!
I admire Mark’s clever and creative mind, careful attention to details, knowledge in so many scientific fields, readiness and ability to work through the math, and perseverance in getting the tedious work done. His down-to-earth attitude and humor are also inspiring. Each time I listen to this book, I find myself trying to emulate these great qualities in my own life. What a wonderful thing, to be so moved by a work of fiction. Though I do like Disco. I’ve been studying about taste buds (at Wikipedia, that favorite source of true knowledge, and a few other sources) and have only just learned that the “taste bud map” concept, of zones on the tongue each responsible for one of the four different tastes, has been debunked. In fact, I learned that taste buds identify (at least) five different tastes: Salty, Sour, Sweet, Bitter, and Umami, a Japanese word meaning ‘savory’ – and those receptors are scattered not only on the tongue but all through the mouth.
I’ve found that I taste more when the food starts at the front of my mouth. I theorize, if you’re able to put food into your mouth with a utensil, you’re delivering it onto the tongue just behind the front teeth, and it has to travel past many taste buds on its way to the esophagus. On the other hand, if you’re getting food through a catheter, generally the food is delivered either to the back/middle of your mouth (if your teeth aren’t fastened shut) or at the far-back-right or -left side of your mouth (if your teeth are fastened shut and you’re running the catheter alongside the teeth). In those cases, the food passes by fewer taste buds – and in my case, it is skipping most of the taste buds that are ‘awake’ and reporting. This has interested me personally, as I realized recently that I am missing many flavors when I eat these days. As I had been trying to interpret my taste sensations according to the taste bud map, I wasn’t able to understand why I felt I was missing something along the hard palate and cheeks. Now that I understand better how taste buds work and are distributed, it has clarified why, when I gulp down a piece of Chef Boyardee “Mini Ravioli”*, and it glides along the roof of my mouth, I taste and feel almost nothing there. That’s just one example; much of the food I am able to eat via utensil travels that same path, and most of it has very little character. Now I understand: the areas in my mouth that are still numb, like the hard palate and the cheeks, are not able to report anything about taste and texture. I’ve been trying to think of a metaphor for how I’m experiencing this food – “… no more character than a lump of mud” or “… no more flavor than a lump of putty”, but have realized that nothing we eat is devoid of flavor and texture. I can’t describe my current experience of sensing no taste and no texture with a metaphor, because it’s unlike anything I have ever experienced. It is true that I can taste those ravioli on my tongue, so it’s not a completely flavorless experience, and I’m thankful for that. But it took me a while to understand why eating has so often been unrewarding. By missing some portion of the flavors and textures, I’m missing some of the built-in pleasure response to eating, which encourages us to eat as we need to. It’s not unusual lately that I have to require myself to eat, intellectually understanding it is necessary to take in food for the calories I need to sustain life and heal (and stave off depression). I sometimes am prompted to eat by hunger. But I am rarely prompted to eat by the anticipated pleasure of eating. This too shall pass, I am sure. More about Swallowing: I have recently come to understand more clearly the struggle I have been having with swallowing since the first day of recovery in the ICU. Having just read more about the amazing, complicated process of swallowing, I understand it better and can track at least some of the actions involved. Many times in this recovery when I’ve tried to swallow mucous or a last bit of food, I’ve felt that I couldn’t complete the swallowing process in the normal way. In particular, the muscles under the mandible (which I believe were stretched and shifted due to the genioplasty, poor things) feel numb and awkward when I swallow. I’ve theorized that some of these muscles that should be active in this process are numb and passive, and that those muscles that are working have to somehow make up for the others’ absence. However, when I asked my surgeon about this theory, he noted that the nerves involved in my surgery were sensory nerves, not motor nerves, and that my swallowing functions have not been impaired: this is just a sensation that I am having. Unfortunately, it seems that the sensations I’m having of some difficulty swallowing are leading me to try to “help” using muscles that have nothing to do with the process. I can often catch muscles in the back of my neck tensing up as I swallow. I’m not sure if that’s a primary reason why those neck muscles are much more rigid and tense than usual right now; I haven’t identified other behaviors yet that might be contributing. I’ll give my Alexander Technique training credit for helping me identify this unnecessary muscular work, but haven’t felt that I have been successful in using it to let go of those patterns very well. While I’m on the topic of the neck, I also realized recently that my front-of-neck muscles experienced their own trauma through the surgery and recovery. We could see yellowish areas on my neck for several days after the surgery – which I understand, perhaps imperfectly, were bruising related to the surgery. My surgeon said something to the effect that “gravity has an effect” on the bruising, and I gathered that it was ‘drifting down’ from the surgical sites and collecting in my neck. It seems my bruising was better than the norm, but it’s still something my neck has had to endure, along with continuing numbness under the jaw. I pet the muscles there every once in a while, but don’t have any idea how to encourage their healing. :) I’m conscious that I’m working too hard at swallowing whenever I’m aware of it. If I don’t have a completely “successful swallow”, I’m left with just a little remnant of the bolus (mostly mucous, I think), hovering in the pharynx, in a distracting and uncomfortable way. Perhaps this is a normal condition of life, and I have just made myself hypersensitive to it. On the other hand, I recall experiencing this sensation at many other times of my life, so it’s not just because of the surgery. Another mystery… Speaking of swallowing, and food that’s NOT helpful: I’ve tried a few wedges of Laughing Cow Cheese. This is very smooth processed cheese, meant to be a tasty treat. Instead, they are torture!, and I think my experience is something like that of a dog with peanut butter in its mouth. I theorize: when you can eat cheese with a cracker, the tongue uses the dryer bits of cracker as a tool to gather up the viscous cheese into a bolus that will hold together as it is pushed by the swallowing mechanism to the back of the throat and down. Crackers don’t work well with my no-chew diet, so I’ve just eaten the cheese alone, and hence the only material my tongue has had to work with is the cheese itself. Poor Tongue; it’s very frustrated! It can’t control the cheese, but unintentionally spreads it lavishly across the hard palate and into each nook and cranny of my teeth. It takes a lot of work to get the cheese headed in the right direction, to the esophagus – and once again, I feel my neck muscles getting tense as they work too hard, “helping”. Only 50 calories taken in, and I’m exhausted. Not worth it! Hmm, I might try preparing the cheese by crushing a cracker into bits and somehow combining them… Now, melted cheese of other kinds is great; it slides right down the gullet, no muss, no fuss, no struggle... *”Thank goodness for Chef Boyardee!” (I sing that to myself sometimes.) I continue to have numbness and paresthesia (a sensation of "pins and needles" varying from irritating to painful) in an area surrounding my nose, jaw, lips, and chin. Saturday (8/27) of last weekend I suffered from intense paresthesia, spent most of that day not doing anything but waiting to feel better, and then felt like I had wasted the day with no improvement to show for it. It wasn't until the next day that it dawned on me that I can't spend my days waiting for this to improve before living my life. After that I re-engaged a bit more in the activities of my life, and found that once I was not dwelling on it so much, the irritation and pain receded, somewhat, into the background.
I saw my surgeon a few days later, and commented that I had been trying to assess each day whether there had been any improvement in that pain. He cautioned me that day-to-day assessment is not appropriate for nerve regeneration, because this kind of healing takes much longer. Rather, we can assess on a monthly basis, or perhaps twice a month. He said, people who look for improvement in this area day to day just end up driving themselves crazy. Hearing this was a bit of a blow. Though it wasn't the first time he had told me of this, it was finally hitting home for me, and I realized that this is yet another challenge to be patient. Around that same time I had also been torturing myself with the fear that I might be among the small percentage of people who have permanent nerve damage, and that this condition will never improve for me. Statistics say that 85% of patients recover fully – but what about that other 15%? My counselor helped me consider this fear when we met last week. We reaffirmed my belief that I have an excellent surgeon who did a wonderful job in my surgery and who I trust when he tells me it's going to take a long time to heal. Also my counselor pointed out there are statistics about people having accidents while driving a car or flying in an airplane, and I don't spend time living in fear of those possible outcomes or let them stop me from driving or flying. If I answer his question, "Who would I be without that thought?" (without that fear), I realize I would be more relaxed, comfortable, and happy. So, I think I'll stay there, and I’m happy to say I have let go of that fear. I am thinking about ways of being pro-active, though -- just a bit. My surgeon OK'd light touching of my face, just saying "hello" to the soft tissues and stimulating the nerves, not disturbing the healing work of the bones, etc. I won't call it "massage" because that implies too much depth and pressure. But loving touch - from myself, from Lorraine, from my parents, from anyone who wants to! - is all good, I think. I can't say that the nerves feel "better" as a result of such touching: I think that looking for results like that takes me right back into the trap of trying to identify and gauge short-term improvements. But I feel better, and I trust that all those good vibrations and good energy are beneficial for me, even if I don't know how. Kind of like prayer, I suppose. I'm still finding material to write about regarding my experience in the hospital, and working it in as I have time. In this post I’ll address several sources of discomfort that I experienced while recovering in the ICU. It does seem to me that there is a host of people who have experienced all these discomforts and many worse ones – so who am I to write with any authority about this? What I do have is a growing passion that thoughtful and thorough information on any given medical issue be made available and actively presented to patients. I’ll hope to make my small contribution to the information and perspective available on the internet, encouraging potential patients to learn about what they are in for and ask questions of their surgeons, to help prepare as best they can.
To start, I’d like to follow up on a post I recently made in which I discussed some ways I've experienced feelings of suffocation in the past, and talk about how I drew on this experience as I was waking from my surgery. Once again I found myself struggling with similar feelings of suffocation and other problems with breathing, though now with a larger set of complicating factors. First, as I woke up the morning after my surgery I was acutely aware, intellectually if not tangibly, of the intubation that I knew had been threaded down my nose, through my vocal cords, and into my trachea to ensure the flow of oxygen through the surgery and initial recovery period. I had had conversations with my surgeon and anesthesiologist in which I expressed unease with intubation, specifically with the possibility of damage to my vocal cords. I understood that intubation was necessary and wasn't at all arguing against it; I was just expressing my concern to the professionals involved. I was appreciative that my anesthesiologist, hearing my concern about my voice, offered to use the smallest size tubing to help make less impact on the vocal cords. I believe that at least some of my unease came from 'anecdotal' information about damage to vocal cords (especially for singers), which I probably didn't understand fully and certainly couldn't tell you the source for, and also from a lack of knowledge about intubation itself. As a pro-active patient who usually informs himself very carefully, I am surprised now at the degree to which I remained ignorant and fearful on this topic. Looking into it now, I see that vocal cord damage is listed in reputable sources as a possible result of intubation. But though there is cause for caution, I have no information about how often it happens or the degree of damage, and it’s possible that if I had researched it more deeply before the surgery, I still would not have been able to gather enough information to feel more confident about that aspect of the procedure. I believe I did what I could in expressing my concern to the surgeon and anesthesiologist, that they responded to my concern, and that I’ve come out the other side with no apparent damage done. But, there in the recovery room, coming out of anesthesia, I remained frightened and uninformed. As I woke up in the ICU, I only became aware of myself and my parts gradually - so that, though I was awake at 7:30 a.m., I didn't realize I had a tongue until 9:30, became aware of the roof of my mouth a couple of hours later, sensed the length of my tongue a little later, and discovered the back of the pharynx later still. Like in those dental appointments of the past, I became aware of water, blood, or saliva that I felt I needed to do something with, but now didn't know what to do with it. I was afraid to try to swallow it because I knew that would force the vocal cords to try to close over the tube, since part of their function is to close off the trachea from anything being swallowed. It was only later that I learned of the balloon cuff near the end of an intubation tube which forms a seal preventing anything from getting into the trachea and the lungs (except the air flowing through the tube itself). At the time, I could feel the liquid rattle of something vibrating on my vocal cords – a deeply disturbing feeling, because I “knew” that meant I was in danger of breathing something liquid into my lungs. I couldn't cough it up and swallow it, and I couldn't do anything else about it either. Now, I understand that the cuff was preventing the liquid from entering my lungs – but I didn’t understand it then, and thought perhaps my breathing was compromised. I was able to write a note to the nurses about this fear, and they were able to set my mind at ease to some degree, though I still didn’t know about the balloon cuff. Also, when that liquid was present, the nurses would run another small tube into my other nostril and all the way down to the larynx (I think), where they could suction it out. My surgeon had carefully taught the ICU nurses how to do this when I came out of surgery (as Lorraine looked on), taking my pharyngeal flap into consideration and carefully maneuvering past it. I found that I could cooperate with this procedure by taking a very slow, careful, long breath and then coughing the liquid up, which helped collect it where it could be suctioned up more effectively. As time went on, I began to notice that different events made me fearful and likely to tense up. Using my Alexander Technique training, I often gave myself directions to release the tension as much as I was able, and even at times to inhibit the inclination to tense in the first place. - At some points while I was intubated, I felt like I was suffocating because I couldn’t breathe right. I had to settle myself down, think through it, and realize that the air was coming in through the tube, and that I had nothing to fear. I also had to inhibit any intention to phonate, and even had to inhibit a tendency towards curiously "checking" whether I could feel the tube anywhere. ("No, Adam, you really don't want to feel that.") - I had a blood pressure cuff on, which tightened to take my blood pressure every hour on the hour. I don't like the feeling of a tight cuff anytime, and in the circumstances (as I was somewhat out of it) I wondered if the pressure was cutting off the blood to my arm and even somehow interfering with blood flow in my whole body. - Both arms were restrained to the bed, as I had three IVs and the intubation, and it was important that I not inadvertently disturb any of them. Most of the time I was at peace with the restraints, but every once in a while I felt restrained and was disturbed about it. - Throughout the night (after I was extubated), while I was trying to sleep, it seemed that every time I felt myself starting to slide into sleep, a monitor beeped near my head. A nurse invariably appeared within a few seconds, checked the readouts, and turned off the alarm. I was thankful to be under such careful observation, but wished the darn alarm would stop going off just when I was finally starting to drift off. - My extubation (taking the intubation out) was a singularly unpleasant experience. I couldn't believe how long the tube was as the doctor drew it out of me. I don't know how you would prepare yourself for this. The (other) ICU doctor holding my hand comfortingly helped. It felt as if my soul was being pulled out of my stomach through my nose. (And Lorraine said it reminded her of the alien-coming-out-of-the-stomach scene in Alien.) Enough said. In many of these circumstances I was able to calm myself in short order. But each occasion that I experienced panic or fear was exhausting, physically and emotionally. I have wondered if it would have been helpful for me to have known more about what I was experiencing in advance. Something like "Your Guide to Staying in the ICU!". Maybe that exists on the internet - everything else does - but I haven't gone looking for it, and certainly hadn't before the surgery. Well, as with other posts I've written, perhaps reading this will prompt a patient to ask questions in advance, and learn a few answers to help him or her find a little more ease during the recovery. All this said, I would like to affirm again - and briefly discard anonymity - to say that the ICU staff at Overlake Hospital in Bellevue were tremendously helpful, competent, and caring for me when I was there. I've realized that though I wrote a very basic description of what was going to be done in my surgery, including the titles of the procedures - Maxillary Osteotomy, Mandibular Osteotomy, Genioplasty (Chin), Septoplasty & Inferior Turbinectomy (Nose) - there's a big difference between knowing the names and actually seeing what goes on. My family and I have watching some videos on YouTube that illustrate what was done to me. If you have the stomach for it - when they bring out the sawz-all and demonstrate cutting the mandible, that was just a bit much for me, even though it's just an animation - these are very interesting videos. Here's a video for prospective jaw surgery patients, showing the basics of what is done in different cases. In my case, the section from 3:58-5:00 shows what was done to me. Another short video showing roughly the same thing. At 1:30 the video shows something like my case, though in this example only the mandible (lower) is adjusted, while for me both the maxilla (upper) and mandible (lower) were advanced. Here's one addressed to surgeons in training, helping them learn the procedure. Shows more detail, though just in animation. Still not for the faint of heart! Now I'll also include a photo of an x-ray of me, post-surgery. In the photo, you can see my braces and a few crowns that replaced some molars. The rest of the hardware that shows up in the x-ray is titanium brackets and screws holding the advancement together. You can see they have been used for my mandible, maxilla, and chin as well. If you watch any of the videos, you can see demonstrations of hardware just like this being used. I look at those screws that are in my bones, and I think, "No wonder my face hurts!" 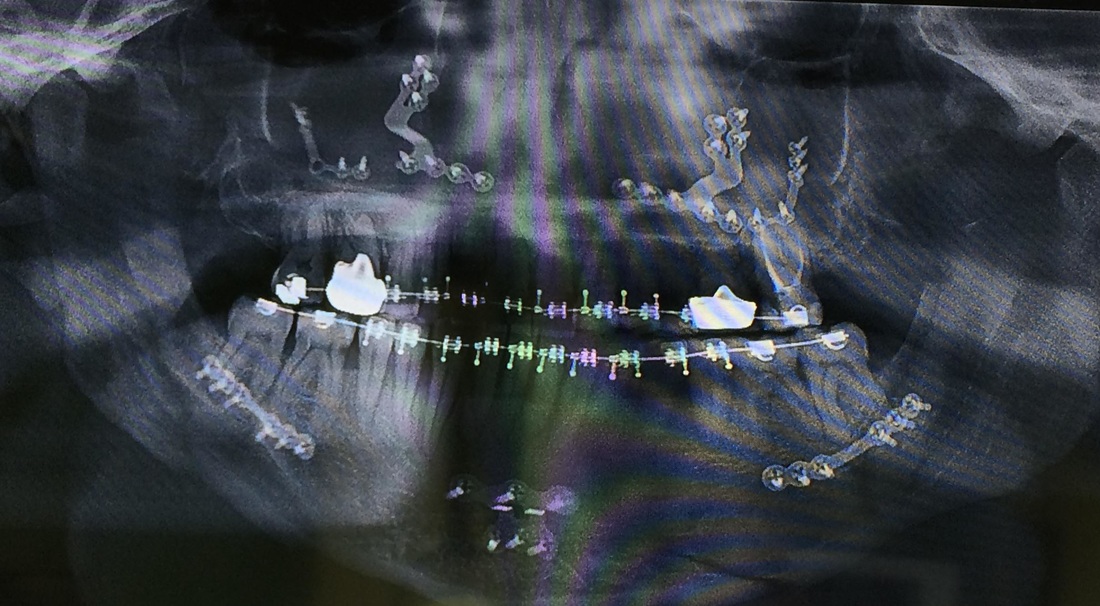 |
AuthorDr. Adam Burdick has been a professional musician for over two decades. Teaching, conducting, and performing in various music genres, he is also a perpetual student with interest in a wide range of topics. He loves to ponder and share his discoveries with anyone interested! Archives
April 2017
Categories |
 RSS Feed
RSS Feed